

 Introduction
Introduction
Ultraviolet (UV) light for air and water germicidal disinfection has been around for quite some time. The 1903 Nobel Prize for Medicine was awarded to the physician who developed UV light to successfully treat skin tuberculosis[i]. It was used in the 1930’s to fight measles in schools and again in the late 1980’s and early 1990’s to combat a resurgence in drug resistant tuberculosis (TB).
With the rapid rise of the COVID-19 pandemic in recent months there has been much media and general discussion around cures, treatments, and prevention solutions. This blog summarizes and analyzes topics presented in the Illuminating Engineering Society’s webinar, “Germicidal Ultraviolet Disinfection in the Days of COVID-19.” If you wish to view the webinar yourself, it has been temporarily published in full at no charge.
What We Know
In laboratory settings, UV lighting has been shown to be highly effective in de-activating airborne viruses such as TB, SARS, and MERS[ii]. UV lighting can pose significant harm to humans in the form of skin burn, skin cancer, eye irritants, and cataracts. Exposure to certain wavelengths and prolonged and direct exposure to eyes and skin are mainly what present these risks. These negative effects can be mitigated by the proper design and implementation of UV systems. More detail will be provided on this later.
In laboratory settings, upper room UV air disinfection systems have been shown to reduce transmission of TB amongst guinea pigs by 70%[iii]. There are not studies at this point showing the effectiveness of UV lighting in the prevention of airborne illness in humans in a hospital or other public setting.
What Types Of UV Disinfection Approaches Exist?
Several technologies exist that designed to disinfected indoor air and surfaces for viruses and bacteria. They are summarized as follows:
Upper Room: studied and agreed among industry and academic experts to be the most effective application of airborne germicidal disinfection. Also relatively economic.
In-Duct: less effective at airborne germicidal disinfection. Highly effective at minimizing bacterial and fungal buildup on heat exchange coils which does improve indoor air quality and has a significant impact on energy efficiency.
Whole Room: perhaps effective when properly implemented at disinfecting surgical rooms between patients. Ineffective / impractical for spaces that cannot be vacated frequently.
Hand Wands: effective for surface decontamination but highly subject to human error and pose high risk to human operator and nearby occupants.
Room Air Filters: ineffective at providing sufficient air changes to achieve a significant air disinfection impact.
Personal Protection: Disinfects PPE successfully but degrades equipment such as N95 masks and gowns very rapidly. Other non-UV methods may be more appropriate for disinfecting soft-goods. UV potentially better for disinfecting equipment that does not degrade as rapidly such as metal hand tools.
222 NM UV: Wavelength of UV light that has less risks associated with direct skin and eye exposure than 254 nm. Effectiveness on inactivating viruses and manufacturing feasibility is still being studied.
Upper Room Germicidal UV
As the above list highlights, Upper Room Germicidal UV (URGUV) systems are agreed to be the most effective in reducing airborne viruses and other contaminants. For this reason, the remainder of this post will focus on how URGUV systems work.
The UV spectrum is the portion of the radiation spectrum that exists between 100 nanometer (nm) wavelengths and 380 nm wavelengths. (Visible light exists between 380 nm and 740 nm.) UV wavelengths between 315 and 280 nm have not been shown to be effective at killing bacteria and deactivating virus. UV wavelengths between 280 and 315 have shown to effectively achieve these tasks. However, these wavelengths also cause skin cancer, skin burn, and eye damage (e.g. cataracts). UV wavelengths between 250 and 260 nm have been shown to have a strong germicidal effect and do not pose a significant skin cancer or skin burn risk. However, they do pose some skin irritants, eye irritants, and eye damage when overexposed[iv].
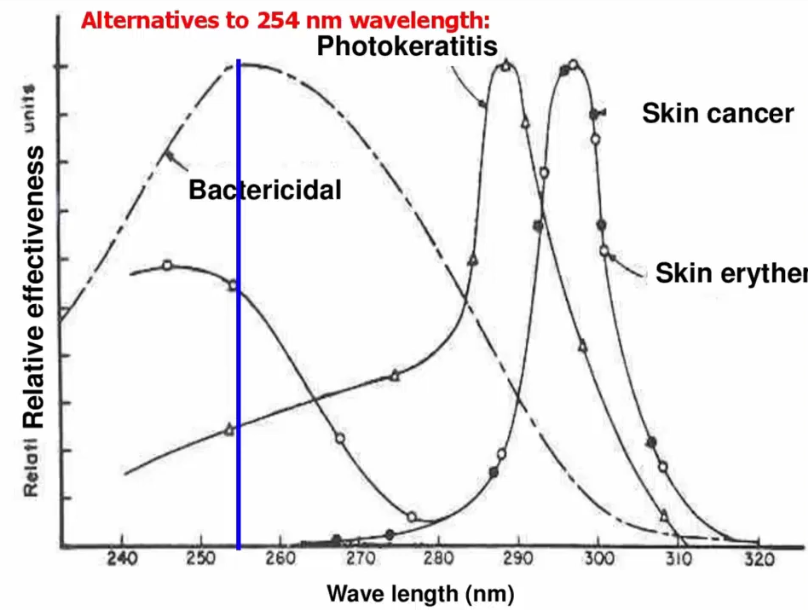
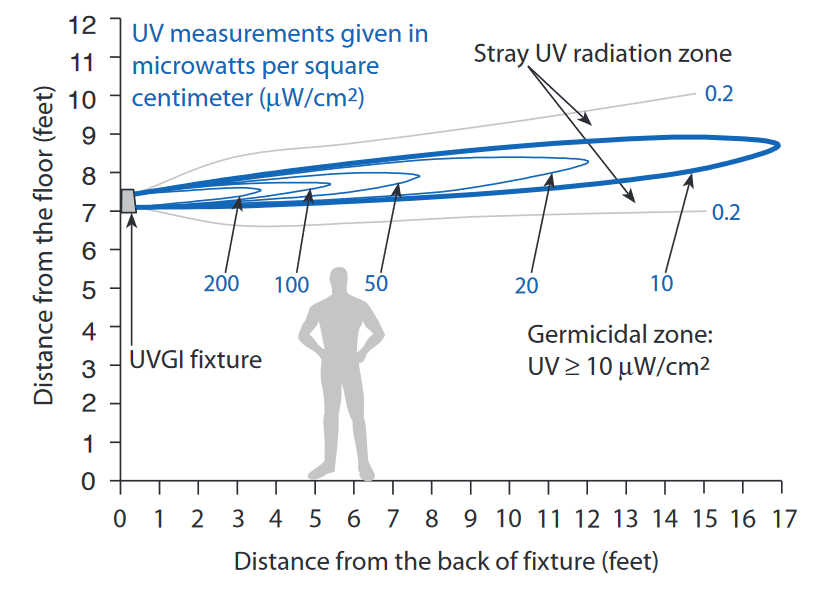
With those items in mind, UV light concentrated in at the 254 nm wavelength has been shown to be highly effective in killing airborne bacteria and viruses. Upper room systems use this light type and are mounted at 7 feet and above to disinfect the air in the upper portion of room (see picture below[v]). So long as the room has a moderate amount of air mixing, the entire volume of air in the room will be decontaminated several times per hour.
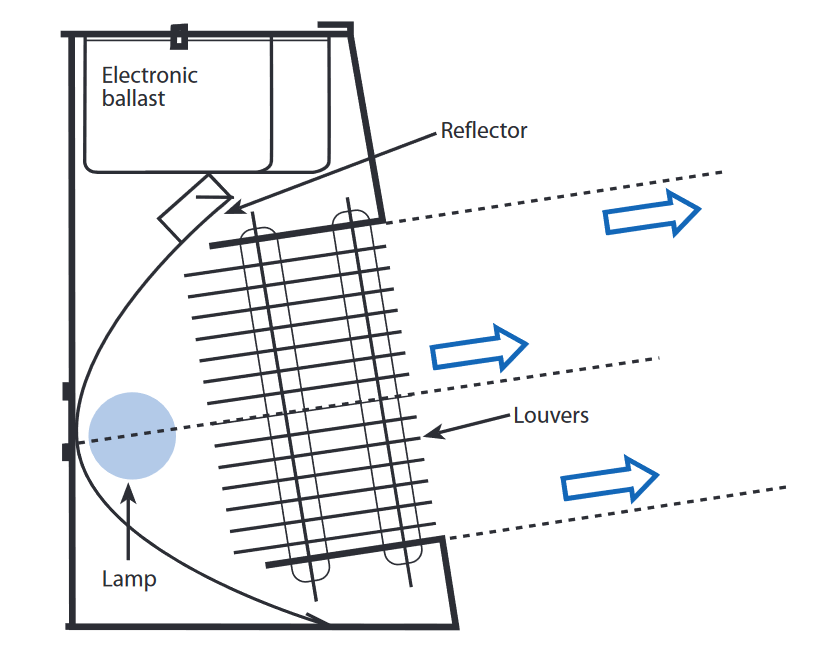
The main risk of a UV light that emits in the 254 nm region is eye and skin irritants. To prevent these negative effects, most URGUV systems are mounted above head level and designed with louvers to prevent UV light from spilling downward towards space occupants (see picture below[vi]).
What are potential application areas?
Any indoor areas with a high concentration of people and/or high percentage of potentially contagious people.
- Hospitals
- Waiting Rooms
- Emergency Departments
- Operating Rooms
- Autopsy Rooms
- Nursing Homes
- Transportation Hubs
- Airports
- Subway stations
- Train stations
- Malls
- Restaurants
- Schools
- Houses of Worship
- Auditoriums
- Sports Stadiums
- Refugee Centers
- Homeless Shelters
- Military Barracks
Can LED lights be used for Germicidal UV?
Thus far there has been limited success for LED to achieve UV light emission in the safe germicidal region of 240 to 260 nanometers. Some products have been developed in the 270 – 280 nm region, but these are only for manual surface decontamination and decontamination of unoccupied rooms.
Summary
There is significant data to support the idea that Upper Room Germicidal UV light systems could reduce transmission of airborne viruses in high risk spaces. Laboratory studies have shown UV light to deactivate viruses such as SARS, MERS, and TB and have also shown to reduce transmission of TB among guinea pigs. No studies have been completed to examine the reduction of transmission of viruses among humans in a real-world setting or have been completed to show the de-activation impact of UV light on COVID-19.
In this author’s opinion, URGUV systems are not a 100% cure for viral epidemics and pandemics such as COVID-19. However, along with other simple measures such as social distancing, masks, and hand washing; such technology could create a significant reduction in the disruptive impact viral airborne diseases have in the future.
This post has been a summary from the author’s perspective of the information presented in the Illuminating Engineering Society’s webinar, “Germicidal Ultraviolet Disinfection in the Days of COVID-19.” If you wish to view the webinar yourself, it has been temporarily published in full at no charge. Related FAQs can be found also be found here
NEWS UPDATE:
NYC Subway Experiments with “Whole-Room” UV Disinfection
NYC Bakery Implements 222 nm UV Disinfection
References
[i] https://www.nobelprize.org/prizes/medicine/1903/summary/
[ii] https://medtradex.com/assets/Uploads/Literature-UVD-Corona.pdf
[iii] https://pubmed.ncbi.nlm.nih.gov/19296717/
[iv] https://www.ies.org/standards/committee-reports/
[v] https://ultraviolet.com/wp-content/uploads/downloads/2015/12/980904.pdf
[vi] https://ultraviolet.com/wp-content/uploads/downloads/2015/12/980904.pdf